
Optimal vasopressor sequencing in septic shock with concurrent right ventricular failure
Sharma P (AIIMS Delhi), Iyer R (CMC Vellore), Kapoor M (NIMHANS), Nair A (Narayana Health), +4 contributors
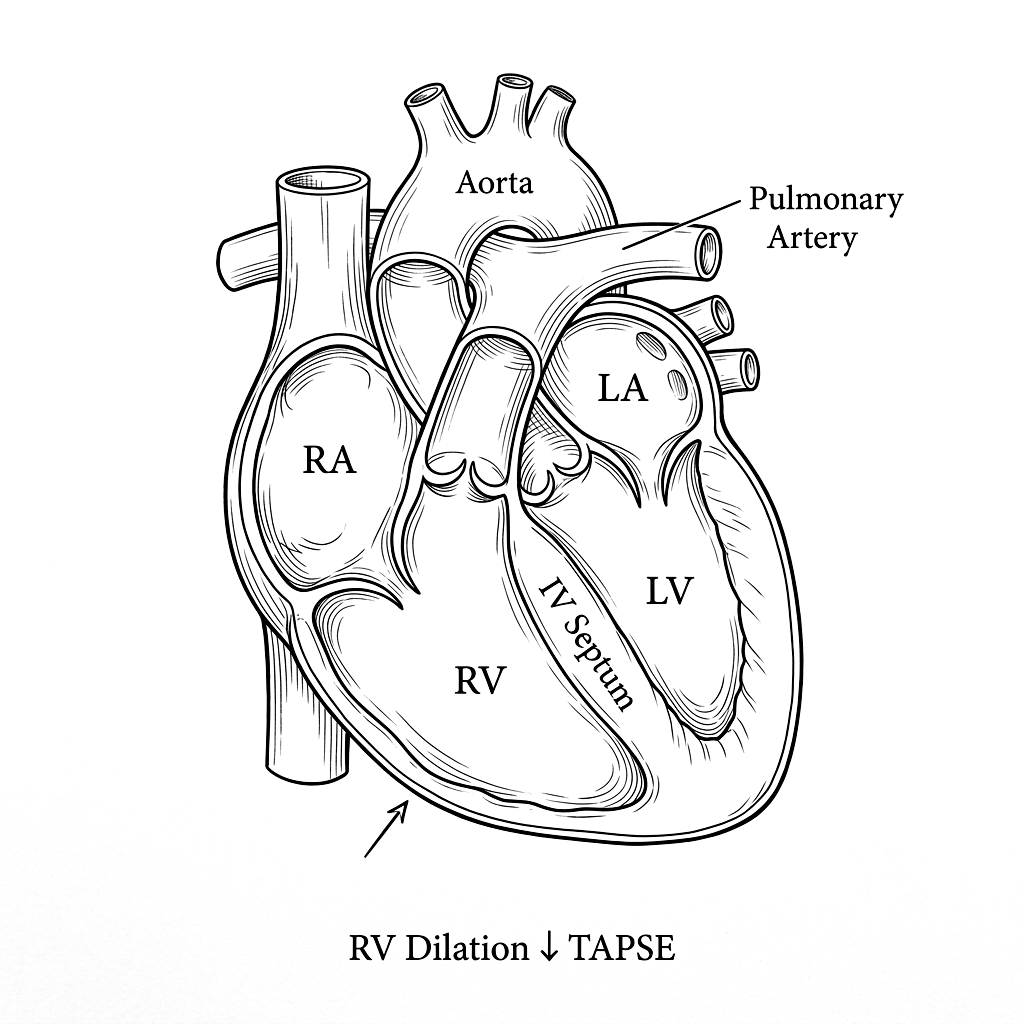
A 58 year old male presented with community acquired pneumonia rapidly progressing to septic shock. Initial resuscitation with 30 mL/kg crystalloid was followed by persistent hypotension (MAP 55 mmHg). Norepinephrine was initiated. Bedside echocardiography revealed severe RV dilatation and dysfunction (TAPSE 12mm1, D-shaped septum2) with preserved LV systolic function. McConnell sign3 was positive. Serum lactate4 increased from 4.2 to 6.8 mmol/L. The optimal vasopressor strategy in this setting of RV dominant shock is debated.
Central venous pressure was 18 mmHg with a CVP waveform showing prominent V waves. Troponin-I peaked at 2.4 ng/mL. Procalcitonin was 28 ng/mL. Blood cultures grew Streptococcus pneumoniae. The team initiated vasopressin at 0.03 U/min as a second vasopressor, followed by inhaled nitric oxide at 20 ppm for selective pulmonary vasodilation. Norepinephrine was weaned from 0.4 to 0.15 μg/kg/min over six hours. Repeat echocardiography at 12 hours demonstrated improved TAPSE (16mm) and resolution of septal bowing.
Lactate clearance was 42% at 6 hours and normalized by 24 hours. The patient was extubated on day 4 and discharged on day 9 with preserved biventricular function. This case underscores the importance of early RV assessment in septic shock and the role of vasopressin-first strategies when RV failure complicates the clinical picture.